Claim denials are among the most significant challenges facing healthcare practices today, directly impacting revenue cycle performance and financial stability. The CO 16 denial code represents one of the most frequently encountered rejection reasons in medical billing. It accounts for substantial revenue delays across the healthcare industry.
Understanding the CO 16 denial code is essential for medical practices seeking to optimize their revenue cycle management. It helps reduce administrative overhead and accelerate reimbursement timelines. This comprehensive guide explores everything billing professionals, doctors, healthcare practice managers, and medical coding team administrators need to know about CO 16 denials. We’ll cover everything from root causes to prevention strategies.
What is the CO 16 Denial Code?
The CO 16 denial code is a Claim Adjustment Reason Code (CARC) that indicates a claim lacks information that is needed for adjudication. The CO prefix designates this as a Contractual Obligation adjustment. This means the provider is financially responsible for the denied amount based on the contractual agreement with the payer.
When a claim receives a CO 16 code, the insurance company is communicating that they cannot process the claim due to missing, incomplete, or invalid information. This denial appears on Explanation of Benefits (EOB) statements and Electronic Remittance Advice (ERA) documents. It typically comes accompanied by specific Remittance Advice Remark Codes (RARCs) that provide additional context about the exact problem.
Impact of CO 16 Denials Code on Cash Flow
CO 16 code creates a major financial burden on healthcare organizations. Beyond delayed revenue, these denials lead to hidden costs, such as extra staff time spent fixing claims, slow cash flow that affects daily operations, lower payment rates when claims miss filing deadlines, and more patient billing issues when claims are wrongly denied.
Research shows that reworking a denied claim costs between $25 to $117 per claim. The exact cost depends on the complexity and resources required for resolution. For practices experiencing high volumes of CO 16 denial codes, when they add up, these costs create serious financial losses.
Causes of CO 16 Denials
Understanding why CO 16 denials occur is the first step toward prevention. These denials occur due to various billing and submission errors, each require specific attention and correction strategies.
1. Missing or Incomplete Patient Demographics
Patient demographic errors most commonly trigger for CO-16 denials. Several issues fall into this category such as missing or incorrect date of birth, invalid or expired insurance identification numbers, incomplete patient name information, missing or inaccurate address details, and incorrect subscriber relationship codes.
2. Authorization and Referral Issues
Many insurance plans require prior authorization for specific procedures, services, or referrals to specialists. CO 16 denials frequently result from several authorization-related problems: missing prior authorization numbers, expired authorization codes, authorization numbers that don’t match payer records, services performed outside the authorized date range, and referrals from providers not recognized in the payer’s network.
Healthcare practices must maintain effective authorization tracking systems to ensure all required approvals are obtained before service delivery and accurately documented on claims.
3. Provider Information Errors
Accurate provider data is critical for claim processing. Several provider-related issues commonly cause CO 16 denials: missing or invalid National Provider Identifier (NPI) numbers, incorrect provider taxonomy codes, mismatched rendering provider and billing provider information, facility NPI issues for institutional claims, and outdated provider enrollment status with the payer.
Practices should regularly audit their provider information across all payer systems to ensure consistency and accuracy, particularly after provider additions, departures, or credential updates.
4. Service Location and Place of Service Errors
The place of service (POS) code identifies where services were rendered and must align with the service type and billing requirements. Common POS-related CO 16 denials include mismatched POS codes and procedure codes, missing facility information for services rendered in institutional settings, invalid facility NPIs, and incorrect POS codes for telehealth services.
5. Diagnosis and Procedure Code Mismatches
Insurance companies evaluate whether submitted procedure codes are medically necessary based on the accompanying diagnosis codes. CO 16 denials occur when diagnosis codes don’t support the medical necessity of billed procedures, ICD-10 codes are too vague or nonspecific, the diagnosis-to-procedure relationship violates payer policies, or required secondary diagnosis codes are missing.
6. Modifier Errors
Procedure code modifiers provide additional information about services rendered, and their incorrect use commonly triggers denials. Issues include missing required modifiers for bilateral procedures or multiple procedures, inappropriate modifier combinations, modifiers that contradict other claim elements, and outdated modifiers no longer recognized by payers.
7. Electronic Claim Submission Errors
Even when claim content is accurate, technical submission issues can cause CO 16 denials. These technical problems include invalid file formats or claim transaction structures, missing required electronic data interchange (EDI) segments, clearinghouse rejection due to formatting errors, and corrupted data transmission.
If you are interested in knowing about the claim insurance card numbers, Checkout our detailed blog on Decoding Insurance Card Numbers To Avoid Costly Billing Mistakes
Commonly Used Remark Codes Associated With CO-16 Denials
When a claim is denied with a CO-16 code, the denial itself only tells part of the story. The real insight comes from the Remittance Advice Remark Codes (RARCs) that accompany it. These remark codes explain what specific information is missing, invalid, or incomplete, allowing medical billing teams to correct claims accurately and avoid repeated denials.
Below are some of the most frequently reported remark codes seen alongside CO-16 denials and what they typically mean in real-world billing scenarios.
Remark Code M12 – Missing Purchased Service Details
Remark Code M12 indicates that the claim involves diagnostic testing, but does not clearly identify whether purchased services were included. Payers require transparency when diagnostic services are outsourced or purchased from another entity.
This denial usually occurs when purchase-related details are omitted or improperly reported on the claim. To resolve it, review the diagnostic service documentation and ensure that all required purchase indicators and details are correctly entered before resubmitting the claim.
Remark Code M60 – Missing Certificate of Medical Necessity (CMN) or DIF
M60 signals that required documentation, such as a Certificate of Medical Necessity (CMN) or a DME MAC Information Form (DIF) is missing or not properly linked to the claim.
This is especially common in durable medical equipment (DME) billing. For example, when a rental item like a wheelchair transfers from another supplier, a new or updated CMN may be required. If the documentation is incomplete or not attached correctly in the billing system, the claim will be denied. Resolution involves attaching the correct CMN or DIF and resubmitting the claim promptly.
Remark Code N264 – Invalid or Missing Ordering Provider Name
Remark Code N264 indicates that the ordering provider’s name is missing, incomplete, or invalid. This often results from data entry errors or discrepancies between the claim and payer enrollment systems, such as PECOS.
Claims for DME items are particularly sensitive to this issue. Ensuring that the ordering provider’s name is entered exactly as it appears in payer records can prevent unnecessary denials under this code.
Remark Code N575 – Ordering or Referring Provider Name Mismatch
N575 points to a mismatch between the provider name submitted on the claim and what the payer has on file. This can occur due to spelling variations, outdated enrollment records, or recent provider credentialing changes that haven’t been updated across systems.
To prevent this denial, practices should routinely verify that provider enrollment information is current and consistent across all billing platforms and payer databases.
Remark Code M124 – Missing Equipment Ownership Information
Remark Code M124 applies when claims for replacement parts, accessories, or supplies lack documentation proving the patient owns the base equipment.
This scenario commonly affects Medicare claims when the original equipment was not billed through Medicare. In these cases, the claim must include the HCPCS code for the base item, confirmation that the patient owns the equipment, and the date the equipment was originally received. Without this information, the claim is considered incomplete and denied.
Step-by-Step Guide to Resolving CO 16 Denials
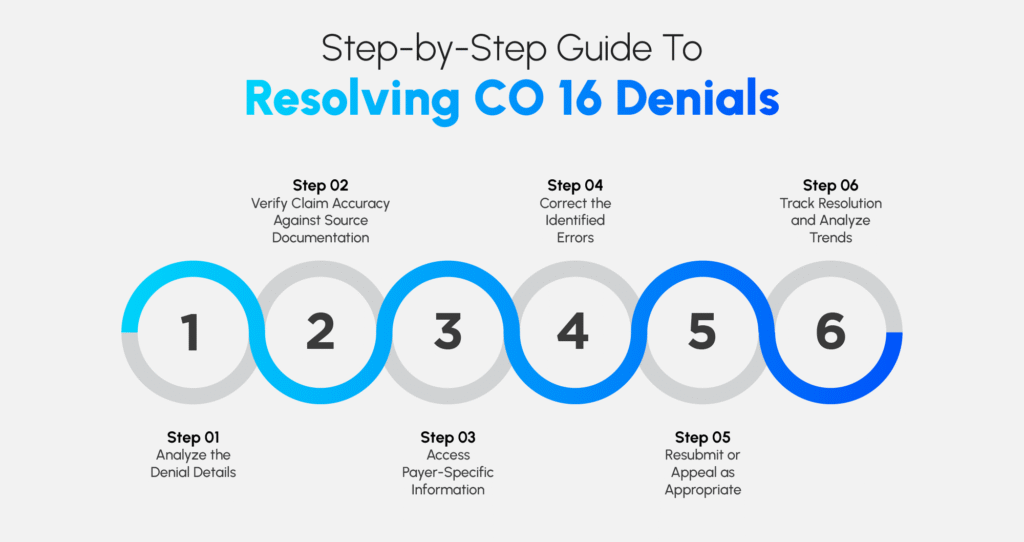
When a CO 16 denial occurs, systematic resolution minimizes revenue loss and prevents future occurrences. Follow this comprehensive workflow to address denials efficiently.
Step 1: Analyze the Denial Details
Begin by thoroughly reviewing the EOB or ERA to identify the specific reason for denial. Look for accompanying Remittance Advice Remark Codes that provide additional context beyond the CO 16 designation. Common RARCs paired with CO 16 include N130 for missing prior authorization, N52 for missing or invalid patient identification, and MA130 for missing referring provider information.
Document all denial details, including the claim number, patient name, date of service, denied amount, specific reason codes, and any payer notes or instructions. This documentation creates an audit trail and helps identify patterns in denial trends.
Step 2: Verify Claim Accuracy Against Source Documentation
Cross-reference the denied claim against your source documentation, including patient registration forms, insurance verification records, authorization documentation, medical records, and provider information. This verification identifies whether the error originated from incorrect data entry, missing information in your records, or legitimate gaps in documentation.
Step 3: Access Payer-Specific Information
Log in to the insurance company’s provider portal to access detailed claim status information, which often provides more specific guidance than the standard EOB. Many payers offer real-time eligibility verification tools, authorization tracking systems, claim submission checklists, and payer-specific coding policies that can clarify denial reasons and correction requirements.
Step 4: Correct the Identified Errors
Based on your analysis, make the necessary corrections. For missing information, gather the required data from patient records, authorization systems, or provider enrollment files. For incorrect information, update claim fields with accurate data verified against authoritative sources. For authorization-related denials, obtain retroactive authorization if the payer permits or submit appeals with supporting clinical documentation.
Ensure corrections address the root cause rather than just the symptom. For example, if a patient’s insurance ID was incorrect, update both the claim and your practice management system to prevent future denials.
Step 5: Resubmit or Appeal as Appropriate
Determine whether the claim should be corrected and resubmitted or if an appeal is necessary. Corrected claims work best when information was genuinely missing or incorrect. They’re appropriate when the claim can be processed with the corrected data. Appeals become necessary when you believe the denial was issued in error. They’re also needed when required documentation was submitted but not acknowledged. Additionally, disputes over payer policy interpretation call for appeals.
For resubmissions, use the appropriate claim type code such as Claim Type 7 for corrected claims, include all corrected information clearly documented, and attach any supporting documentation requested by the payer. For appeals, prepare a formal appeal letter explaining the dispute, compile all supporting documentation including authorization letters and medical records, submit within the payer’s specified timeframe, and maintain copies of all appeal submissions.
Step 6: Track Resolution and Analyze Trends
Monitor resubmitted and appealed claims through to final adjudication. Track days in accounts receivable for CO 16 denials, resolution success rates, most common denial reasons within the CO 16 category, and payer-specific denial patterns.
Use this data to identify systemic issues requiring workflow improvements, staff training needs, or payer-specific challenges requiring escalation.
Preventing CO 16 Denials: Proactive Strategies
Prevention is significantly more cost-effective than denial management. Implementing robust front-end processes eliminates most CO 16 denials before claims are submitted.
Implement Comprehensive Front-End Verification
Establish standardized processes for patient registration and insurance verification at every patient encounter. Verify active coverage and benefits, confirm patient demographic information matches insurance records, identify authorization requirements for scheduled services, and validate provider network participation. Use automated eligibility verification tools that integrate with your practice management system to streamline this process and reduce manual errors.
Utilize Automated Claim Scrubbing Technology
Modern claim scrubbing software identifies potential denial triggers before claim submission, including missing or invalid data elements, authorization requirements, coding inconsistencies, and payer-specific edit failures. Configure your scrubbing software with current payer rules and regularly update these parameters as policies change.
Best-in-class claim scrubbing solutions reduce submission errors by 50-70%, significantly decreasing CO 16 denial rates and improving first-pass claim acceptance.
Maintain Accurate Provider and Payer Data
Establish a formal process for maintaining provider enrollment and credentialing data. Conduct quarterly audits of NPI and taxonomy code accuracy across all payer systems, update provider information immediately following credential changes, maintain current contracts and fee schedules with all payers, and document provider enrollment status for new payers before billing services.
Develop Robust Authorization Management Workflows
Create systematic processes for obtaining, tracking, and documenting authorizations. Identify authorization requirements during appointment scheduling, submit authorization requests with sufficient lead time before service dates, track authorization approval status and expiration dates, document authorization numbers in both clinical and billing systems, and establish alerts for authorization expirations requiring renewal.
Consider implementing authorization tracking software that integrates with your electronic health record and practice management systems to centralize authorization management.
Invest in Staff Training and Education
Regular staff education prevents knowledge gaps that lead to billing errors. Provide ongoing training covering payer-specific billing requirements, current coding guidelines and updates, proper modifier usage, authorization procedures, and common denial causes and prevention strategies.
Leverage Revenue Cycle Management Analytics
Use RCM analytics to monitor key performance indicators related to CO 16 denials including clean claim rate, first-pass acceptance rate, denial rate by payer and denial reason, average days to denial resolution, and percentage of denied claims successfully overturned.
Establish benchmarks and set improvement targets. Then use data to drive continuous process enhancement.
Consider Outsourcing Strategic Functions
Many healthcare practices take benefit from outsourcing the revenue cycle to experienced companies. Professional billing services providers like Liberty Liens offer expertise in medical billing, Payment posting, medical coding, AR follow-up, and denial management to handle volume fluctuations without staffing constraints.
Liberty Liens your outsourcing partner, assesses your practices. We provide tailored services aligned with your specific specialty and payer mix.

Clean Claim Submission Checklist
Use this comprehensive checklist before submitting claims to ensure completeness and accuracy.
1. Patient Demographics
Full legal name matching insurance card, accurate date of birth, complete current address, correct insurance ID and group number, and proper subscriber relationship designation.
2. Provider Information
Valid billing provider NPI and taxonomy code, correct rendering provider NPI and specialty, accurate referring provider NPI when applicable, facility NPI for institutional claims, and proper service location information.
3. Service Documentation
Appropriate place of service code, accurate CPT and HCPCS codes, correct ICD-10 diagnosis codes supporting medical necessity, proper modifier usage, and accurate service dates.
4. Authorization and Coverage
Valid prior authorization number when required, authorization dates encompassing service dates, verification of active coverage on service date, confirmation of benefits for services rendered, and network status verification.
5. Billing Details
Correct claim type designation, appropriate bill type code for institutional claims, accurate charges and units of service, and proper linking of diagnosis codes to service lines.
When to Appeal a CO 16 Denial
“Not all CO 16 denials require appeals. However, certain situations warrant formal dispute. Consider appealing when you have documentation proving all required information was included on the original claim, the payer’s system failed to recognize properly submitted data, authorization was obtained but not recorded in the payer’s system, or payer policy appears to have been misapplied.
Building a Strong Appeal
Successful appeals require thorough documentation and clear communication. Prepare a detailed appeal letter that references the specific claim and denial reason, clearly states why the denial was inappropriate, cites relevant policy language supporting your position, and provides a specific request for claim reprocessing.
Attach comprehensive supporting documentation, including copies of authorization letters or forms, verification of benefits documentation, medical records supporting medical necessity, provider enrollment verification, and any communication with the payer regarding the claim.
Submit appeals according to payer-specific requirements, including designated appeal addresses or portal submissions, required forms or templates, specified timeframes typically 30 to 180 days from denial date, and any special formatting or documentation requirements.
Technology Solutions for CO 16 Prevention
Modern healthcare technology offers powerful tools to reduce CO 16 denials through automation and real-time verification.
1. Practice Management Systems
Contemporary PMS platforms include built-in claim scrubbing, real-time eligibility verification, authorization tracking modules, automated coding assistance, and integrated denial management workflows.
2. Revenue Cycle Management Software
Specialized RCM platforms provide advanced analytics identifying denial patterns, automated claim status checking and follow-up, rules-based claim editing and validation, payer-specific requirement databases, and workflow automation for common corrections.
3. Artificial Intelligence and Machine Learning
Emerging AI technologies offer predictive denial prevention by analyzing historical data patterns, intelligent coding suggestions based on documentation, automated authorization prediction and submission, and natural language processing of medical records for coding accuracy.
Investing in appropriate technology generates significant return on investment. Benefits include reduced denial rates, faster reimbursement cycles, decreased administrative costs, and improved staff productivity.
Measuring Success: Key Performance Indicators
Track these metrics to assess your CO 16 denial management performance.
1. Denial Rate
Calculate the percentage of submitted claims denied with CO 16 codes. Industry benchmarks suggest best-performing practices maintain denial rates below 5%, with CO 16 denials representing less than 1% of total submissions.
2. Clean Claim Rate
Measure the percentage of claims paid upon initial submission without any denial or rejection. Target clean claim rates of 95% or higher.
3. Average Days to Resolve Denials
Track the time between denial receipt and successful resolution. Efficient processes resolve CO 16 denials within 7-14 days.
4. Denial Overturn Rate
Calculate the percentage of appealed CO 16 denials successfully overturned. Rates above 60% suggest effective appeal processes.
5. Revenue Recovery
Measure dollars recovered from denied claims. This metric demonstrates the financial value of your denial management efforts.
Regular monitoring of these KPIs enables data-driven process improvements. Moreover, it demonstrates the value of denial prevention investments.
Conclusion
The CO 16 denial code, while common, is largely preventable. Success comes through systematic processes, staff education, and appropriate technology investments. By understanding the root causes of these denials and implementing comprehensive prevention strategies, healthcare practices can significantly improve their revenue cycle performance.
Success requires commitment to several key areas. Front-end verification forms the foundation. Ongoing staff training keeps skills current. Regular process audits identify improvement opportunities. Leveraging technology enables automation and analytics. Whether you manage billing in-house or partner with external RCM specialists, focus on prevention rather than remediation. This approach achieves optimal financial outcomes.
Remember that every prevented CO 16 denial represents more than just recovered revenue. It also means reduced administrative burden, improved cash flow, and enhanced practice efficiency. Make denial prevention a strategic priority. Your practice will reap the benefits through stronger financial performance and streamlined operations.
By mastering CO 16 denial management, you position your practice for sustainable financial success in an increasingly complex healthcare reimbursement environment.